When is it needed?
Indications- • Cancer of the esophagus (food pipe)
- • Selected junction cancers (esophagus–stomach)
- • Severe, non-cancer conditions rarely (case-by-case)
Patient Guide
This page explains the surgery in simple terms — what it means, why it’s needed, the pre-surgery tests, and what recovery looks like. If you are considering robotic / minimally invasive esophagectomy in Mumbai, this guide will help you understand the typical journey and recovery.
For suitable patients, minimally invasive / robotic approach can mean:
Illustrative (not patient-specific). Suitability depends on tumour stage and overall fitness.
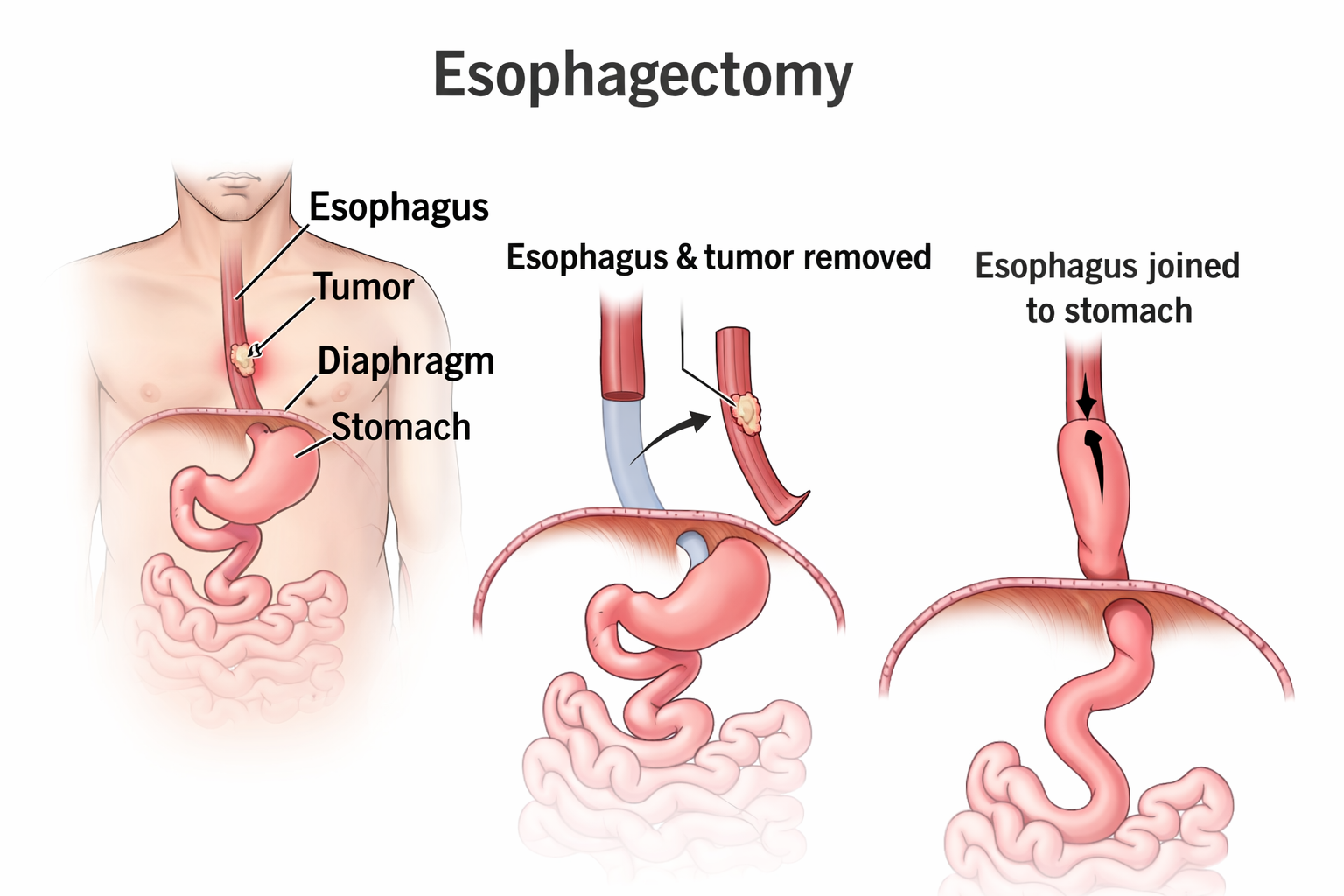
An esophagectomy is an operation to remove part (or occasionally all) of the esophagus — the “food pipe” that carries food and liquids from your throat to your stomach. It is most commonly performed for esophageal cancer and selected cancers at the esophagus–stomach junction.
During surgery, the diseased segment is removed and the digestive pathway is reconstructed so you can swallow again. In cancer cases, nearby lymph nodes are also removed for accurate staging.
The approach depends on where the tumor is located, your overall fitness and the technique that offers the best balance of safety and cancer clearance.
Your surgeon will explain the rationale for the recommended approach and what it means for recovery time.
Open surgery uses larger incisions to access the chest and/or abdomen. Minimally invasive (laparoscopic/thoracoscopic) and robotic approaches use smaller incisions with camera guidance. For suitable patients, this may reduce pain and speed up mobilization, while maintaining oncologic principles.
Surgical details vary by patient. This page is general information and does not replace medical advice.
After surgery, it is common to feel tired and have reduced appetite initially. Some patients experience reflux, bloating or loose stools as the body adapts. Important risks include lung infection (pneumonia), leak at the join (anastomotic leak), bleeding, infection and blood clots. Your team monitors closely to reduce these risks.
Local search note (Mumbai)
If you are searching for robotic esophagectomy in Mumbai, bring your endoscopy report, biopsy and CT/PET scans. A personalised plan is made after reviewing staging and fitness assessment.
Day 0–2
ICU monitoring, pain control, breathing exercises
Day 3–5
Walking, physiotherapy, tubes gradually reduced
Week 1–2
Stepwise diet plan, home care instructions
Weeks 4–6
Improving stamina, follow-up + pathology discussion
Watch video
Tip: Tap full-screen for easier viewing.
Download brochure
Download and keep a copy with your medical records. Easy to print and written in patient-friendly language.
Most operations take about 3–6 hours, depending on the technique and complexity.
A temporary feeding tube is commonly used after surgery to support nutrition while swallowing heals.
Many patients stay 7–14 days, but this varies based on recovery and any complications.
Diet usually progresses step-by-step: feeding tube → liquids → soft foods, guided by your team and dietitian.
Not always. Suitability depends on tumor stage/location and your overall fitness. Your surgeon will advise the safest approach.
Respiratory complications (like pneumonia) are among the most common—breathing exercises and early walking help reduce risk.
Endoscopy and biopsy reports, CT/PET images (CD/pen drive), medication list, and any prior treatment details.
Go to the ER if you cannot breathe or swallow, have severe chest pain, or vomit blood.
Next step
Bring your reports and scans. We’ll explain options in simple terms and plan safely.